In July 1917, on the eve of the Third Battle of Ypres, the Germans introduced two new chemical weapons to the battlefield. One was a failure, the other a spectacular success. The story of their use illustrates one of the lessons of chemical weapons from the First World War: the impossibility of predicting how they would behave in the field.[1]While gas played a comparatively minor role on the battlefield in 1916, it would become ubiquitous by the end of the following year. Chemical warfare in 1917 was characterised by the British introduction of a new and effective means of delivery for chemical agents, the Livens projector, and by the German introduction of a new agent for artillery shells, mustard gas. This article focuses on the introduction and impact of mustard gas.
All the combatants used colour-coded markings on their shells, and the Germans used a system to simplify the complex varieties of chemical fillings according to their function. The existing diphosgene shells and others containing lethal lung irritant gas, which might dissipate in a few hours and was regarded as non-persistent, were marked with a green cross. In July 1917 as British preparations for the Third Battle of Ypres were underway, the Germans introduced two new chemical agents, neither of which can accurately be described as a gas.

German Blue Cross shell for the 77mm field gun, showing the glass bottle containing the chemical embedded in the explosives.
The first was diphenyl chloroarsine, or Blue Cross. The concept of these shells was not in themselves to cause death or injury, but to penetrate respirator filters with a fine particulate dust, causing uncontrollable sneezing and coughing which would force the wearers to remove their respirator and succumb to lethal diphosgene shell. The ‘mask-breaker’ shells were coded with a blue cross. If effectively disseminated, the arsenic dust could cause intense pain to the sinuses and mental depression. However, two factors served to diminish the effect of these shells. Firstly the Germans chose as their method of dissemination to embed a glass bottle containing the powder in a high explosive shell and this rarely produced particles fine enough to penetrate the British respirator filters. Secondly, the British had already introduced this concept with stannic chloride and, between April and June 1917, had issued a particulate filter as an extension for their respirator to protect their own troops in the Ypres Salient. Moreover, they had under development a new filter box incorporating the filter which they began issuing in July. The Blue Cross shells however had the advantage of being effectively indistinguishable in flight and detonation from normal high explosive shells, thus soldiers had no warning of the bursting of the shells and might succumb before they could adjust their masks.
Strandfest: the first use of Blue Cross at Nieuwpoort, 10 July 1917
The Germans introduced Blue Cross shells during their operation to retake the bridgehead at Nieuwpoort (Nieuport) from which they rightly suspected that the recently-arrived British were to launch an operation along the Belgian coast. They amassed 146 artillery batteries for this small, local action, under the codename Strandfest (which might roughly translate as ‘Beach Party’). Because of bad weather, the attack date was shifted several times, until early on 10 July orders were issued for a ten-hour preparatory bombardment to commence at 10am. In addition to diphosgene (Green Cross) and tear gas shells, the British reported another type which burst like a high explosive shell but caused sneezing, slight irritation of the nose and eyes, and tightness of the chest. At 8pm, the German 3rd Marine Division stormed the British positions and threw them back over the Yser. Despite taking 1,250 British prisoners, the Germans were apparently unable to establish how useful the new Blue Cross shells had actually been in achieving the success.[2]
In order to obtain evidence of the effectiveness of both the Blue Cross shells and the method of combining them with Green Cross, the Germans staged a major raid on 28 July at Wytschaete, south of Ypres. Code-named, Heuernte or ‘Hay Making,’ the operation involved a bombardment of British positions at 10.40pm for six minutes by nine light field howitzer batteries with 100 rounds each of Blue Cross ammunition. This was followed by 14 minutes with high explosives after which five raiding parties entered the British trenches. They found, however, that the British had withdrawn from the shelled area and no prisoners were obtained.
British investigations following the 10 July attack where also inconclusive. There were reports of the new symptoms but they were unable to recover an unexploded shell in order to identify the filling until early August. The more dramatic use of mustard gas, which occurred shortly afterwards on the night of 12-13 July, also delayed investigation into the Blue Cross shells.
The development of Mustard Gas
While Blue Cross was developed as an attack ammunition for use in conjunction with Green Cross, mustard was adopted as a defensive agent which was suitable for the continuous poisoning of an area. Mustard gas, dichlorodiethyl sulphide, is in fact an oily liquid with a low boiling point, given the name mustard gas by the British owing to its odour of mustard or horseradish in its impure form. It was to become the most effective chemical agent used during the First World War owing not to the numbers which it killed but to the temporary effects of skin blistering and severe conjunctivitis and to its ability to render ground uninhabitable owing to the time which it took to evaporate. Its effect on the skin was noted by Viktor Meyer in 1886 and both the British and French considered adopting mustard in 1916 only to reject it on the grounds of its lack of toxicity. Professor Ernest Starling, in charge of British anti-gas research, had ordered experiments on cats in 1916. However, the persistency of mustard, that is, the way that it continued to poison for hours or days after release, was not noticed and the range being only that of a bursting shell, it was turned down.
The Germans named it ‘Lost’ after the names of the proposers in 1916: Dr Wilhelm Lommel at the Bayer research laboratories and Dr Wilhelm Steinkopf at the Kaiser Wilhelm Institute. Trials were carried in September and October 1916 out by Doctors Ferdinand Flury and Curt Wachtel, toxicologists at the Kaiser Wilhelm Institute. Their test results on monkeys demonstrated eye and respiratory injury but made no mention of skin symptoms. Wachtel later described how, in late 1916, mustard came to be adopted. [3] The head of the Kaiser Wilhelm Institute for Physical Chemistry and also head of the German chemical warfare programme, Fritz Haber, learnt from the German commanders Hindenburg and Ludendorff that they required a defensive gas suitable for preventing Allied attacks expected in the summer of 1917. Haber was able to propose the newly-tested mustard gas which would remain dangerous for long after the gas shell then in use had dissipated, and industrial production was initiated. Haber’s son, L F Haber, however suggests that, while mustard was selected because of its persistency, its effect was still expected to be as a lethal lung-irritant rather than the non-lethal casualty producer that it in fact turned out to be: ‘No one appears to have remembered that Meyer, thirty years earlier, had written of its blistering action.’[4]
The lack of lethal effect was in fact noted before it was used in the field, according to Wachtel, following a serious explosion at the Adlershof gas shell filling plant, near Berlin, in the spring of 1917. Occurring after the first 1,200 77mm shells had been prepared, this explosion delayed the first use of mustard by several weeks. But a lack of casualties during the fire fighting and clean up led to claims that it was not sufficiently toxic which had to be refuted with further toxicology tests. A trial was conducted in which 500 mustard shells were fired on a test range on which several hundred cats and dogs were tethered. Before its use in the field, mustard was dismissed by most gas warfare experts as being the best means to kill cats but not as a war gas. [5]

German Yellow Cross mustard gas shell for 105mm howitzer.
The First Mustard Gas Bombardment, 12-13 July 1917
The new shells were marked with a yellow cross to indicate their persistency. The first bombardments which the Germans carried out at Ypres were clearly intended to forestall the British offensive. From the start, mustard was a defensive agent, used to poison areas of ground over which the Germans had no intention of attacking in the foreseeable future. Some 50,000 shells, containing 125 tonnes of mustard, were used on this first night. [6] The bombardment, with 77mm and 105mm shells, was in three phases apparently reflecting the way that non-persistent gas clouds were created and topped up using shells: starting at 10.10pm for twenty minutes, it resumed at 12.30am, again for twenty minutes, followed by a third phase at 1.55am for twenty-five minutes.[7]
On detonation the shells, bursting with a dull plop, sprayed the liquid in a seven-metre radius in the case of the 77mm and about 10 metres in the case of the 105mm.[8] Contact with either the liquid or the vapour, which evaporated in sunlight, caused injury. However, the lack of any immediate symptoms meant that British troops did not keep their masks on and did not appreciate the danger of being present in the vicinity of the shells. At first those in the bombardment suffered only slight irritation of the nose which caused some sneezing (perhaps the result of Blue Cross shells). However, in an hour or two they suffered painful inflammation of the eyes, vomiting, followed by reddening of the skin and blistering.

The first mustard gas bombardment reported in the War Diary of the 45th Infantry Brigade, 12 July 1917. (The National Archives, WO95/1943)
Large numbers of British casualties began to report to medical units to the rear of Ypres. The first were admitted to Numbers 47 and 61 Casualty Clearing Stations at Dozinghem (near Poperinge) and Numbers 46 and 64 at Mendinghem (near Proven) and on 13-14 July a total of 2,143 were admitted to these four units. By the time they reached the Casualty Clearing Station the conjunctivitis had developed so rapidly that they were virtually blind and had to be led in files, each man holding on to the man in front, guided by an orderly or lightly wounded man.
![British_55th_Division_gas_casualties_10_April_1918[1]](https://simonjoneshistorian.com/wp-content/uploads/2014/02/british_55th_division_gas_casualties_10_april_19181.jpg)
British mustard gas casualties at an Advanced Dressing Station, April 1918 (IWM Q 11586).
In the first few hours the symptoms were in strong contrast to those usually found in gas cases, with only one or two casualties suffering from symptoms of acute pulmonary oedema (again this was possibly caused by Green Cross shells mixed with the new shells). The majority suffered little distress to their breathing, although some exhibited a husky voice and a hard cough. After a few more hours, symptoms of laryngitis, tracheitis and bronchitis became more definite in a large number of the cases and some developed grave or fatal broncho-pneumonia. [9]
Men developed blisters on their buttocks, genitals and armpits. Within two days many were suffering from bronchitis and some had died from inflammation of the lungs. By the sixth day the conjunctivitis which caused the blindness had disappeared but the breathing difficulties were still severe and the blistering had been replaced by skin rashes. Of the 2,143 cases admitted to the four Casualty Clearing Stations, a comparatively small number, 95, or 4.4%, died. German unit histories report that the British guns were all but silenced for up to two days.

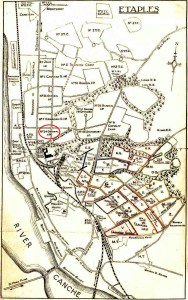
Canadian victim of mustard gas at No.7 Canadian General Hospital, Etaples, c. 1917 (Library and Archives Canada/ Wikimedia).
Up to the end of July, the Germans bombarded the Ypres area every night with mustard, during which the Germans gunners had to surround their own gun positions with chloride of lime as a precaution against leaks or premature bursts of the shells. In addition, a series of set-piece gas shoots were conducted. On 15 July a ‘multi-coloured’ shoot of a thousand rounds was carried out which, despite barrel bursts, was repeated the following day. Then, on 17th and again on 21st, more extensive gas shoots were carried out on tracks, shelters and accommodation at Zillebeke Lake.
On the night of 20-21 July Blue and Green Cross were again tried in combination in an operation called Britentod or ‘British death,’ postponed from the previous night owing to strong winds. British battery positions at Voormezele were targeted, each German field battery having been issued with 900 rounds of Green Cross and each howitzer battery 350 rounds of Blue Cross. The bombardment, from 1am to 3am, completely silenced the British batteries although no mention is made of mustard having been used.
On the same night, in an operation called Totentanz, or ‘Dance of Death,’ Armentières was first targeted with mustard gas, injuring about 6,400. The following night, 21-22 July, Nieuwpoort was heavily bombarded with mustard, thus the south and north flanks successively of the expected British attack area were rendered impassable. The casualties were worse overall than those suffered at Ypres as the troops here had not yet received adequate warning and instructions regarding mustard gas.
On 23-24 July, Britentod was repeated, then on 26-27 gas bombardments in the Wytschaete sector named Schlesien and Apolda. On 28-29 July, renewed gas bombardments of Armentières and Nieuwpoort were carried out between 1am and 4.30am. The civilian casualties from mustard gas in Armentieres totalled 675, of which 86 had died by 18 August, a high mortality due in part to the number of elderly citizens, many living in cellars, who were either unable or reluctant to leave the area while the shelling was in progress.
From July, Blue and Yellow Cross shells were used in very large numbers with a reduction only coming in the winter of 1917-18. Once the Germans had identified the improved protection afforded by the British respirator against Blue Cross, they came to use these shells at the beginning of a gas bombardment, as the shells could not be distinguished from HE shell. The sneezing symptoms would therefore affect men before they could adjust their masks and then cause them to succumb to Green Cross shells used subsequently. HE or Blue Cross shells were also used to disguise the distinctive bursting sound of Yellow Cross mustard gas shells.
During August and September 1917, the Germans used mustard to defeat French attacks on either side of the river Meuse, causing 13,158 to be poisoned and 143 killed. Losses were so great in the affected areas that it has been claimed that the French were forced to abandon the attack.[10] The combination of Green and Blue Cross shells, used for the first time to support the attack at Nieuwpoort on 10 July, was later used for the successful German assault across the Daugava river on 1 September 1917 which lead to the fall of Riga. The artillery fire plan was the work of Colonel Georg Bruchmüller and the publicity accorded it has led some to assume incorrectly that Bruchmüller invented this combination of gas shells, called Buntschiessen or ‘colour shoots’.
Mustard gas caused serious casualties to the British in July 1917 but there seems to be no evidence to support the claim by Beumelburg and Hanslian that it caused the start of the 3rd Battle of Ypres to be postponed for a fortnight.[11] Hanslian and Seesselberg claimed also that it prevented a British break-though during the offensive. However, whilst mustard continued to be used throughout the battle, it was not used to cover the withdrawal of German forces as it would be in 1918, as they could not contaminate ground which they would wish immediately to recapture. Although the Germans improved slightly the effectiveness of their Blue Cross shells, the Allies regarded them as a wasted effort, something that post-war German writers could not accept.
Conclusion: Yellow Cross in 1918
The year 1918 was to see the development of German gas tactics, in particular the use of the persistent mustard gas to block the flanks of areas attacked. The Germans used gas shells in unprecedented numbers and they were integral to their spring and summer offensives. Against infantry, the Green Cross diphosgene and Blue Cross combination was 50% of the total shells used. Against artillery, the ratio was as high as 80% mustard to high explosive. Areas outside the attack zone were heavily shelled with mustard to prevent counter attacks. Mustard was extremely effective as a counter-battery weapon and British decontamination measures broke down. At one point in 1918 the British had the equivalent to two divisions in hospital suffering from mustard gas injuries. However, gas was less effective during the June – July offensives: attacking in gas masks behind a gas barrage was especially fatiguing for the Germans, while Allied casualties were decreasing.
For the remainder of the year, the Germans were in retreat and mustard was to prove far more suited to defence than attack. On 31 July 1918 they used 340,000 mustard gas shells to forestall a Franco-American attack west of Verdun. During September – October British mustard gas casualties were 3 – 4,000 per week but as the British advanced continued, German bombardments became less effective and poorly targeted. It was impossible for the Germans to create their complex fire plans as supply and command became disorganised. When the Allied advances began, the Germans discovered that French troops were less hindered by mustard having learnt to minimise casualties when passing through affected areas. Supplies of mustard were less plentiful by September and during October gas ceased to be a factor in halting the Allied advance.
The cases of both Blue Cross and Yellow Cross shells demonstrate that chemical weapons rarely behave on the battlefield in ways predictable in the laboratory or on the firing range. Nevertheless, the German use of mustard was rightly regarded as a military success. Despite apparently intending its effect to be as a lethal lung irritant rather than a non-lethal casualty producer, mustard revolutionised chemical warfare, and introduced an agent which almost alone amongst the chemical weapons of the First World War has continued application into the 21st century. Until the introduction of mustard, the artillery arm, by far the most flexible means of using gas, had been handicapped by the lack of an agent effective enough in the smaller quantities delivered by shell. By its persistent nature mustard provided this. The German unity of research, production and military expertise, embodied in the person of Fritz Haber, meant that the right substance was available to meet the military demand.
The introduction of mustard gas however was a gamble for Germany. A physicist at the Kaiser Wilhelm Institute, Wilhelm Westphal, claimed that when Haber described mustard gas to General Ludendorff, he warned against its use unless the war was certain to be won within the year. Otherwise the Allies would produce mustard for themselves and Germany lacked the Allies’ ability to replace contaminated uniforms. This alone, he said, could lose the war for Germany. It did take the Allies a year to produce their own mustard gas, achieved by the French through accepting casualties in their factories comparable to those at the front. Westphal’s anecdote may be apocryphal but when the Germans identified French-produced mustard in August 1918, this awareness that the Allies would probably soon be using it on a large scale was one more reason why the Germans would be unable to continue fighting in 1919.
Text (c) Simon Jones. See below for Notes.

Yellow Cross: Measures to protect against mustard gas

Understanding Chemical Warfare in the First World War
Notes on Yellow Cross: the advent of Mustard Gas
[1] This article is an extract from a paper delivered at the In Flanders Fields Museum in 2007 and is partially referenced.
Contact me if you require more information on sources.
[2] W. Volkart,
Die Gasschlacht in Flandern im Herbst 1917, (E S Mittler & Sohn, Berlin, 1957) p.46. The British Official History, J. E. Edmonds,
Military Operations France and Belgium 1917 Vol. II, (HMSO. London, 1948), p. 119, mistakenly states that the Germans used mustard gas in the bombardment prior to this assault.
[3] Curt Wachtel,
Chemical Warfare, (Chemical Publishing Co., Brooklyn, 1941), pp. 226-7.
[4] L. F. Haber,
The Poisonous Cloud, (Clarendon Press, Oxford, 1986), p. 117.
[5] Wachtel,
op. cit., pp. 221-2.
[6] Volkart,
op. cit., citing Rudolf Hanslian,
Der Chemische Krieg, (E S Mittler & Sohn, Berlin, 1937).
[7] Hanslian,
op. cit., pp. 132-141.
[8] Volkart,
op. cit., p.40.
[9] W. G. MacPherson (ed.),
History of the Great War Medical Services Diseases of the War, Vol. II, (HMSO, London, 1923), pp. 292-293.
[10] Hanslian,
op. cit., pp. 132-141.
[11] Hanslian
op. cit., p. 140.







































{kind=link}